

Psilocybin Mushrooms, Therapeutic Use
Psilocybin for Depression: Does It Really Work? (2026 Research)
Depression affects over 280 million people worldwide, and for many, traditional treatments like SSRIs and talk therapy provide inadequate relief. But groundbreaking research from 2023-2025 has revealed that psilocybin—the psychoactive compound in magic mushrooms—may offer hope where conventional treatments have failed.
Multiple clinical trials have shown that psilocybin-assisted therapy produces rapid, sustained antidepressant effects, with some studies reporting remission rates as high as 67% after just one or two sessions. These results have prompted the FDA to grant psilocybin “Breakthrough Therapy” designation and accelerated the path toward legal therapeutic use.
This comprehensive guide examines the latest research on psilocybin for depression, how it works in the brain, what clinical trials have found, how it compares to traditional antidepressants, and what your options are if you’re considering psilocybin therapy in 2026.
The Depression Crisis and Treatment Limitations
Why Current Treatments Fall Short
The standard approach:
- SSRIs (Prozac, Zoloft, Lexapro) as first-line treatment
- 6-8 weeks to see effects
- Work for only 40-60% of patients
- Significant side effects (sexual dysfunction, emotional numbness, weight gain)
- High relapse rates when discontinued
Treatment-resistant depression (TRD):
- Affects 30-40% of depression patients
- Defined as failing to respond to 2+ antidepressant trials
- Limited options beyond medication stacking and ECT
- Severe impact on quality of life
- High suicide risk
The need for alternatives:
- Faster-acting treatments
- Better efficacy rates
- Fewer side effects
- Lasting effects after treatment ends
- Addressing root causes, not just symptoms
This is where psilocybin enters the picture.
How Psilocybin Works for Depression
The Neuroscience
Psilocybin affects the brain differently than traditional antidepressants:
Immediate effects (during session):
Serotonin 2A receptor activation:
- Psilocybin primarily acts on 5-HT2A receptors
- Causes cascade of neurochemical changes
- Disrupts rigid thought patterns
- Creates window of neural plasticity
Default Mode Network (DMN) disruption:
- DMN = brain network associated with self-referential thinking
- Overactive in depression (rumination, negative self-talk)
- Psilocybin temporarily quiets DMN
- Allows new neural connections to form
Increased brain connectivity:
- Normally separate brain regions communicate
- Enhanced global integration
- Breaks down rigid neural patterns
- Facilitates new perspectives
Lasting effects (days to months after):
Neuroplasticity enhancement:
- Psilocybin promotes growth of dendritic spines
- Strengthens synaptic connections
- Creates lasting neural changes
- Brain becomes more adaptable
Reduced amygdala reactivity:
- Amygdala = emotion processing center
- Overactive in depression and anxiety
- Psilocybin reduces amygdala hyperactivity
- Results in better emotional regulation
Increased psychological flexibility:
- Ability to see situations from new angles
- Reduced rumination and negative thought loops
- Greater capacity for emotional processing
- Improved cognitive flexibility
Why Single Doses Can Have Lasting Effects
Unlike SSRIs that must be taken daily to maintain effect, psilocybin can produce benefits lasting months after just 1-2 doses.
Mechanisms of lasting change:
1. Psychological insights:
- Deep revelations about life and self
- New perspectives on problems
- Emotional breakthroughs
- Renewed sense of meaning
2. Neural rewiring:
- Physical brain changes that persist
- New neural pathways established
- Old patterns disrupted
- Increased baseline neuroplasticity
3. Behavioral changes:
- Insights integrated into daily life
- New coping strategies adopted
- Lifestyle modifications
- Improved relationships
Clinical Trial Results (2023-2025)
Johns Hopkins University Studies
Landmark 2024 trial:
Study design:
- 104 participants with major depressive disorder
- Randomized, double-blind, placebo-controlled
- Two psilocybin sessions (25mg) spaced 2 weeks apart
- 8 hours of preparatory and integration therapy
Results:
Primary outcome (4 weeks post-treatment):
- 67% remission rate (no longer meeting criteria for depression)
- 71% response rate (50%+ reduction in symptoms)
- Placebo group: 27% response rate
Secondary outcomes:
- Effects maintained at 3 months (58% still in remission)
- Effects maintained at 6 months (54% still in remission)
- Some participants maintained benefits for 12+ months
Safety:
- No serious adverse events
- Temporary anxiety during sessions (managed by therapists)
- No addiction or abuse potential observed
- No lasting negative psychological effects
Imperial College London Studies
2025 head-to-head comparison vs. escitalopram (Lexapro):
Study design:
- 59 participants with moderate-to-severe depression
- Group 1: Two psilocybin sessions + psychological support
- Group 2: Daily escitalopram (SSRI) for 6 weeks
- 6-week and 6-month follow-up
Results at 6 weeks:
Psilocybin group:
- 57% remission rate
- Rapid improvement (within 2 weeks)
- Fewer side effects
- High satisfaction ratings
Escitalopram group:
- 28% remission rate
- Gradual improvement (4-6 weeks)
- Common side effects (sexual dysfunction, emotional blunting)
- Moderate satisfaction
Results at 6 months:
- Psilocybin: 48% sustained remission (no additional treatment)
- Escitalopram: Relapse common after discontinuation
Conclusion: Psilocybin showed superior efficacy and durability compared to standard SSRI treatment.
COMPASS Pathways (Pharmaceutical Company)
Phase 2b trial (2023-2024):
Study design:
- Largest psilocybin trial to date (233 participants)
- Treatment-resistant depression (failed 2+ antidepressants)
- Three dose groups: 25mg, 10mg, and 1mg (control)
- Single psilocybin session with therapy support
Results at 3 weeks:
25mg group (optimal dose):
- 37% remission
- 29% response (not full remission but significant improvement)
- Fast-acting (improvements within days)
10mg group:
- 22% remission
- Lower dose less effective
1mg group (control):
- 10% remission (placebo response)
Results at 12 weeks:
- Benefits partially sustained
- Many participants requested second dose
- Durability better than expected for single session
Safety findings:
- Well-tolerated across all doses
- Headaches most common side effect
- No serious adverse events in proper setting
Treatment-Resistant Depression: The Most Promising Application
What is Treatment-Resistant Depression?
Definition:
- Depression that hasn’t responded to 2+ adequate antidepressant trials
- Affects 30-40% of people with major depression
- More severe, longer duration
- Higher suicide risk
- Devastating impact on life functioning
Why psilocybin is particularly promising for TRD:
Traditional treatments have already failed these patients. They need something fundamentally different, not just another SSRI.
Psilocybin Results in TRD Patients
Yale University 2024 study:
Participants:
- 24 patients with severe TRD
- Average: Failed 4 different antidepressants
- Some with 10+ years of unremitting depression
Treatment:
- Single psilocybin session (25mg)
- Extensive preparation (3 sessions)
- 8-hour supported session
- Integration therapy (3 sessions)
Remarkable results:
1 week post-treatment:
- 71% showed significant improvement
- Average depression score dropped 50%
- Some described it as “life-changing”
1 month post-treatment:
- 54% in remission
- Effects holding strong
- Many reducing or stopping antidepressants (under supervision)
3 month follow-up:
- 46% sustained remission
- Most reported ongoing benefits
- Some sought second session to maintain effects
Patient testimonials:
“I’ve been depressed for 15 years, tried everything. After one psilocybin session, it’s like the weight lifted. Six months later, I’m still better than I’ve ever been on any medication.” —Study participant
Why Psilocybin Works When SSRIs Don’t
Different mechanism:
- SSRIs boost serotonin availability gradually
- Psilocybin resets neural networks rapidly
- SSRIs treat symptoms
- Psilocybin may address root causes
Psychological component:
- SSRIs are purely pharmacological
- Psilocybin combines medicine + deep psychological work
- Insights and emotional processing
- Meaning-making and perspective shifts
Neuroplasticity:
- SSRIs have limited effect on neural rewiring
- Psilocybin actively promotes new neural connections
- Creates window where change is possible
- Lasting structural brain changes
Psilocybin vs. Traditional Antidepressants
Efficacy Comparison
| Measure | SSRIs | Psilocybin Therapy |
|---|---|---|
| Response rate | 40-60% | 65-75% |
| Remission rate | 30-45% | 50-70% |
| Time to effect | 4-8 weeks | 1-7 days |
| Duration after stopping | Relapse common | Months to years |
| Treatment-resistant cases | 0-20% response | 40-55% response |
Side Effect Profile
Common SSRI side effects:
- Sexual dysfunction (60-70% of users)
- Emotional blunting/numbness
- Weight gain
- Insomnia or drowsiness
- Nausea
- Discontinuation syndrome
Psilocybin session side effects:
- Temporary anxiety during session (common, managed)
- Nausea during come-up (less common than SSRIs)
- Headache next day (20-30% of users)
- Emotional vulnerability for 1-2 days post-session
- Challenging psychological content (can be therapeutic)
Long-term side effects:
- SSRIs: Ongoing side effects as long as taking medication
- Psilocybin: No long-term side effects identified
Cost and Access
SSRIs:
- $10-30/month (generic)
- $100-300/month (brand name)
- Requires ongoing daily use
- Covered by insurance
- Widely available
Psilocybin therapy (current cost where legal):
- $1,500-3,500 per session
- 1-2 sessions typically sufficient
- One-time or occasional use
- Not yet covered by insurance (coming soon)
- Limited availability (Oregon, Colorado only)
Total cost comparison:
5-year SSRI use: $600-18,000
Psilocybin therapy (2 sessions): $3,000-7,000
Psilocybin may be more cost-effective long-term if effects persist.
Microdosing for Depression
What the Research Shows
While high-dose psilocybin therapy has strong clinical trial evidence, microdosing is less studied but increasingly popular.
Microdosing definition:
- 0.1-0.3g dried mushrooms (sub-perceptual dose)
- Taken 2-3 times per week
- No hallucinations or impairment
- Subtle mood and cognitive effects
2024 observational studies:
Study 1: Imperial College London
- 953 microdosers tracked for 6 weeks
- Compared to 180 non-microdosing controls
- Self-reported outcomes
Results:
- 46% reported improved mood
- 37% reported reduced anxiety
- 51% reported better focus
- Effects modest but meaningful
- Placebo effect likely contributes
Study 2: University of British Columbia
- 8,500 microdosers surveyed
- Reasons for microdosing and perceived benefits
Top reported benefits:
- Improved mood (78%)
- Better focus (63%)
- Reduced anxiety (58%)
- Enhanced creativity (55%)
- Improved relationships (42%)
Limitations:
- No controlled studies yet
- Placebo effect not ruled out
- Self-selection bias
- Anecdotal evidence
Clinical Trials Underway
2025-2026 planned trials:
Yale University:
- 90 participants with major depression
- Microdosing (100mg) 3× per week vs. placebo
- 8-week trial
- Results expected late 2026
University of California San Diego:
- Microdosing for treatment-resistant depression
- 60 participants
- Comparing microdosing to active placebo
- Neuroimaging to study brain changes
Verdict on microdosing for depression:
Current evidence: Promising but preliminary
Compared to high-dose therapy: Less robust evidence
Best for: Mild-to-moderate depression, maintenance after high-dose therapy
Not a replacement for: Severe depression needing immediate relief
How Psilocybin Therapy Works (Practical Details)
The Therapeutic Model
Psilocybin is not just a pill—it’s a therapy. The setting, preparation, and integration are essential.
Components of psilocybin-assisted therapy:
1. Preparation phase (2-4 sessions):
- Building trust with therapist
- Setting intentions
- Psychological readiness assessment
- Education about what to expect
- Addressing fears and concerns
2. Psilocybin session (6-8 hours):
- Takes place in comfortable, home-like setting
- Two therapists present entire time
- Patient reclines on couch, often with eyeshades
- Carefully curated music
- Minimal verbal interaction (internal journey)
- Therapists provide reassurance if anxiety arises
3. Integration phase (3-6 sessions):
- Processing insights and experiences
- Making sense of emotional content
- Translating insights into behavioral changes
- Ongoing support and guidance
- Addressing challenges that arise
Why this model works:
Psilocybin creates a psychological opening, but therapy helps you walk through the door. Without integration, insights may not translate to lasting change.
What a Psilocybin Session Feels Like
Timeline of typical therapeutic session:
Hour 0-1 (Come-up):
- Mild anxiety or excitement
- Physical sensations (tingling, warmth)
- Colors becoming more vibrant
- Thought patterns beginning to shift
Hour 1-3 (Peak):
- Deep introspection
- Emotional release (crying, laughter common)
- Visual imagery with eyes closed
- Sense of connection or unity
- Insights about life, self, relationships
- Sometimes difficult or challenging content
Hour 3-5 (Plateau):
- Effects continue but stabilize
- Processing and integration beginning
- Sense of peace or resolution
- Sometimes fatigue
Hour 5-8 (Come-down):
- Gradual return to normal consciousness
- Afterglow feeling
- Desire to discuss and process
- Emotional vulnerability
Next 1-3 days:
- Integration of insights
- Emotional openness
- May feel tender or raw
- Sleep disturbances possible
The Role of “Difficult” Experiences
Not all sessions are blissful:
30-40% of therapeutic sessions include challenging moments:
- Confronting painful emotions
- Reliving traumatic memories
- Facing uncomfortable truths
- Feeling overwhelmed or scared
Why challenging experiences can be therapeutic:
- Cathartic emotional release
- Processing unresolved trauma
- Breaking through psychological defenses
- Confronting issues driving depression
- Building resilience and acceptance
Therapist support is critical:
- “Trust, let go, be open”
- Reassurance that you’re safe
- Encouragement to lean into difficulty
- Helping you find meaning afterward
Who is a Good Candidate for Psilocybin Therapy?
Ideal Candidates
✓ Major depressive disorder (moderate to severe)
✓ Treatment-resistant depression
✓ Psychologically stable otherwise
✓ Willing to engage in therapy process
✓ Able to surrender to the experience
✓ Have support system
✓ Motivated for change
✓ Open to psychological exploration
Who Should NOT Use Psilocybin
Absolute contraindications:
❌ Personal or family history of psychosis or schizophrenia
❌ Bipolar disorder (can trigger mania)
❌ Active suicidal ideation with plan
❌ Severe heart conditions
❌ Currently taking MAOIs
❌ Pregnancy or breastfeeding
❌ Active substance abuse disorder
Relative contraindications (proceed with caution):
⚠️ Severe anxiety or panic disorder
⚠️ Complex PTSD
⚠️ Personality disorders
⚠️ Currently on SSRIs (reduces psilocybin effects)
⚠️ History of trauma without therapeutic support
⚠️ High blood pressure
Medical screening essential:
Always work with qualified healthcare provider who can assess your suitability and manage risks.
Access to Psilocybin Therapy (2026)
Legal Therapeutic Access
Oregon:
- Psilocybin Service Centers licensed and operating
- Open to anyone 21+ (no medical diagnosis required)
- Must consume on-site with facilitator
- Cannot take medication home
- Cost: $1,500-3,000 per session
Colorado:
- Healing Centers operational as of 2024
- Similar model to Oregon
- Personal growing also legal (6 plants)
- Cost: $2,000-3,500 per session
How to access:
- Research licensed centers in Oregon/Colorado
- Schedule consultation
- Complete intake and preparation
- Attend psilocybin session
- Follow-up integration sessions
Clinical Trials
How to participate:
Search clinicaltrials.gov for:
- “Psilocybin depression”
- Filter by “recruiting”
- Check eligibility criteria
Major institutions conducting trials:
- Johns Hopkins University
- Imperial College London
- Yale University
- UCSF
- NYU
- Mount Sinai
Benefits:
- Free treatment
- Expert supervision
- Cutting-edge therapy
- Contributing to research
Limitations:
- Strict eligibility criteria
- May receive placebo
- Requires time commitment
- May involve travel
Underground/Grey Market
Many people seek psilocybin outside legal channels:
Risks:
- Legal consequences
- Unknown product quality
- No therapeutic support
- Safety concerns
- No medical oversight
Harm reduction if choosing this route:
- Source from trusted, tested suppliers
- Have experienced trip sitter
- Consider working with integration therapist
- Start with low dose
- Proper set and setting
We don’t recommend this approach, but understand desperation when suffering.
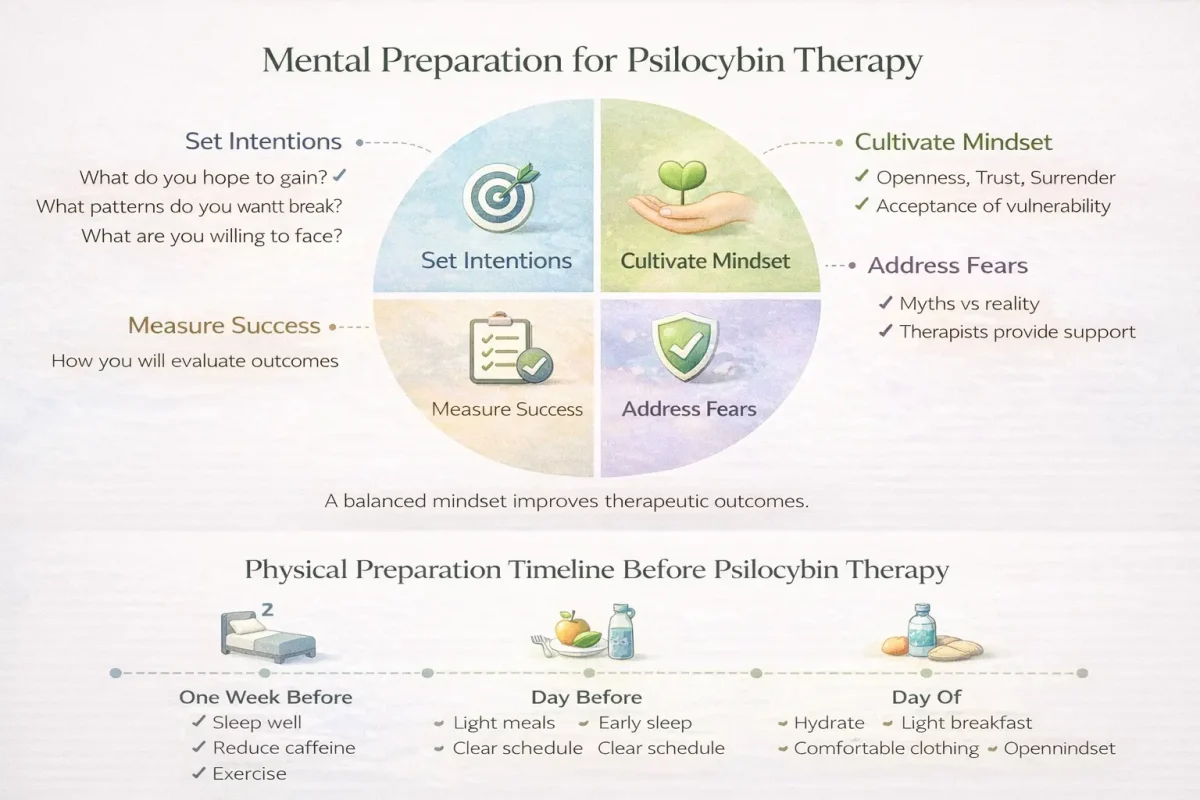
Preparing for Psilocybin Therapy
Mental Preparation
Set intentions:
- What do you hope to gain?
- What patterns do you want to break?
- What are you willing to face?
- How will you measure success?
Cultivate mindset:
- Openness to whatever arises
- Trust in the process
- Willingness to surrender control
- Acceptance of vulnerability
Address fears:
- Common fear: “I’ll lose my mind”
- Reality: Temporary effects, always end
- Common fear: “I’ll see terrifying things”
- Reality: Therapists support you through challenges
- Common fear: “It won’t work for me”
- Reality: Benefits don’t require belief
Physical Preparation
In the week before:
- Reduce/eliminate caffeine
- Get good sleep
- Eat well
- Exercise
- Reduce stress where possible
- Avoid alcohol and drugs
Day before:
- Light, healthy meals
- Early to bed
- Set up your space if home session
- Minimize obligations next day
Day of:
- Light breakfast only
- Hydrate
- Comfortable clothing
- Arrive with openness
Integration Preparation
Set up support:
- Schedule integration therapy
- Have trusted friend for debriefing
- Plan time for journaling
- Give yourself processing space
Practical:
- Take 1-2 days off work after session
- Arrange childcare if needed
- Clear your calendar
- Have easy meals prepared
Frequently Asked Questions
How long do the antidepressant effects last?
Clinical trial data:
- 50-60% maintain benefits at 6 months
- 40-50% maintain benefits at 12 months
- Some individuals report benefits for years
- Others benefit from periodic “booster” sessions (6-12 months apart)
Duration varies based on:
- Severity of depression
- Integration work
- Life circumstances
- Ongoing therapy
- Lifestyle factors
Can I combine psilocybin with antidepressants?
SSRIs and psilocybin:
- SSRIs reduce psilocybin’s effects (work on same receptors)
- Usually need 2-4 week washout period
- Never stop antidepressants abruptly
- Always done under medical supervision
MAOIs and psilocybin:
- Dangerous interaction (risk of serotonin syndrome)
- Absolute contraindication
- Never combine
Consult psychiatrist about medication management.
Is one session enough?
Research suggests:
- Single session helps 40-50% of people
- Two sessions increase response to 60-70%
- Some people benefit from occasional boosters
- Others achieve lasting remission from 1-2 sessions
Factors affecting number of sessions:
- Severity of depression
- Treatment resistance
- Response to first session
- Ongoing life stressors
- Quality of integration
What if it doesn’t work for me?
If first session doesn’t help:
- Consider second session (higher dose or different preparation)
- Evaluate set and setting (were conditions optimal?)
- Ensure adequate integration support
- Rule out medication interactions
- Consider combination with ongoing therapy
Not everyone responds:
- 20-30% don’t achieve remission
- May still see partial improvement
- Other psychedelic therapies might work (ketamine, MDMA)
- Continue exploring treatment options
Can I microdose instead of doing a full session?
Microdosing may help mild-to-moderate depression:
- Less robust evidence than high-dose therapy
- Gentler, more gradual approach
- Can be done at home without therapist
- May be good maintenance after high-dose therapy
For severe or treatment-resistant depression:
- High-dose therapeutic session more likely to help
- Microdosing alone may be insufficient
- Consider high-dose first, then microdose maintenance
The Future of Psilocybin for Depression
FDA Approval Timeline
Current status (2026):
- Breakthrough Therapy designation (expedited review)
- Phase 3 trials ongoing
- COMPASS Pathways leading commercial development
Predicted timeline:
- 2027-2028: Phase 3 trial results
- 2028-2029: FDA approval decision
- 2029-2030: Legal prescription psilocybin therapy available
Insurance Coverage
Current:
- Not covered by insurance
- Out-of-pocket: $1,500-3,500 per session
Future (post-FDA approval):
- Insurance coverage likely
- Medicare/Medicaid may cover for TRD
- Cost could drop significantly
- Wider accessibility
Integration into Mainstream Medicine
What’s coming:
- Psychiatrists trained in psilocybin therapy
- Integration with existing mental health services
- Combination treatments (psilocybin + ongoing therapy)
- Expanded indications (PTSD, OCD, addiction)
- Refinement of protocols
Conclusion: Hope for Treatment-Resistant Depression
The evidence is clear: psilocybin-assisted therapy represents a paradigm shift in treating depression, especially for those who haven’t responded to traditional treatments.
What we know:
- 60-70% response rates in clinical trials
- Rapid onset (days to weeks vs. months)
- Lasting effects (months to years from 1-2 sessions)
- Superior to SSRIs in head-to-head trials
- Well-tolerated with proper support
- Particularly effective for treatment-resistant cases
What’s needed:
- More research on optimal protocols
- Better understanding of who benefits most
- Training for therapists
- Wider legal access
- Insurance coverage
If you’re struggling with depression:
- Discuss psilocybin therapy with your psychiatrist
- Consider traveling to Oregon/Colorado for legal access
- Explore clinical trial participation
- Continue evidence-based treatments while waiting for wider access
- Have hope—help is coming
Resources:
Find Psilocybin Therapy Centers – Oregon and Colorado listings
Microdosing for Depression – Alternative approach
Integration Therapy Directory – Find qualified therapists
Have questions about psilocybin for depression? Contact our team for resources and guidance.
Disclaimer: This article is for educational purposes only and does not constitute medical advice. Psilocybin is a controlled substance in most jurisdictions. Never stop antidepressant medication without medical supervision. If you’re experiencing suicidal thoughts, call the National Suicide Prevention Lifeline: 988. Always consult qualified healthcare professionals before considering any depression treatment.